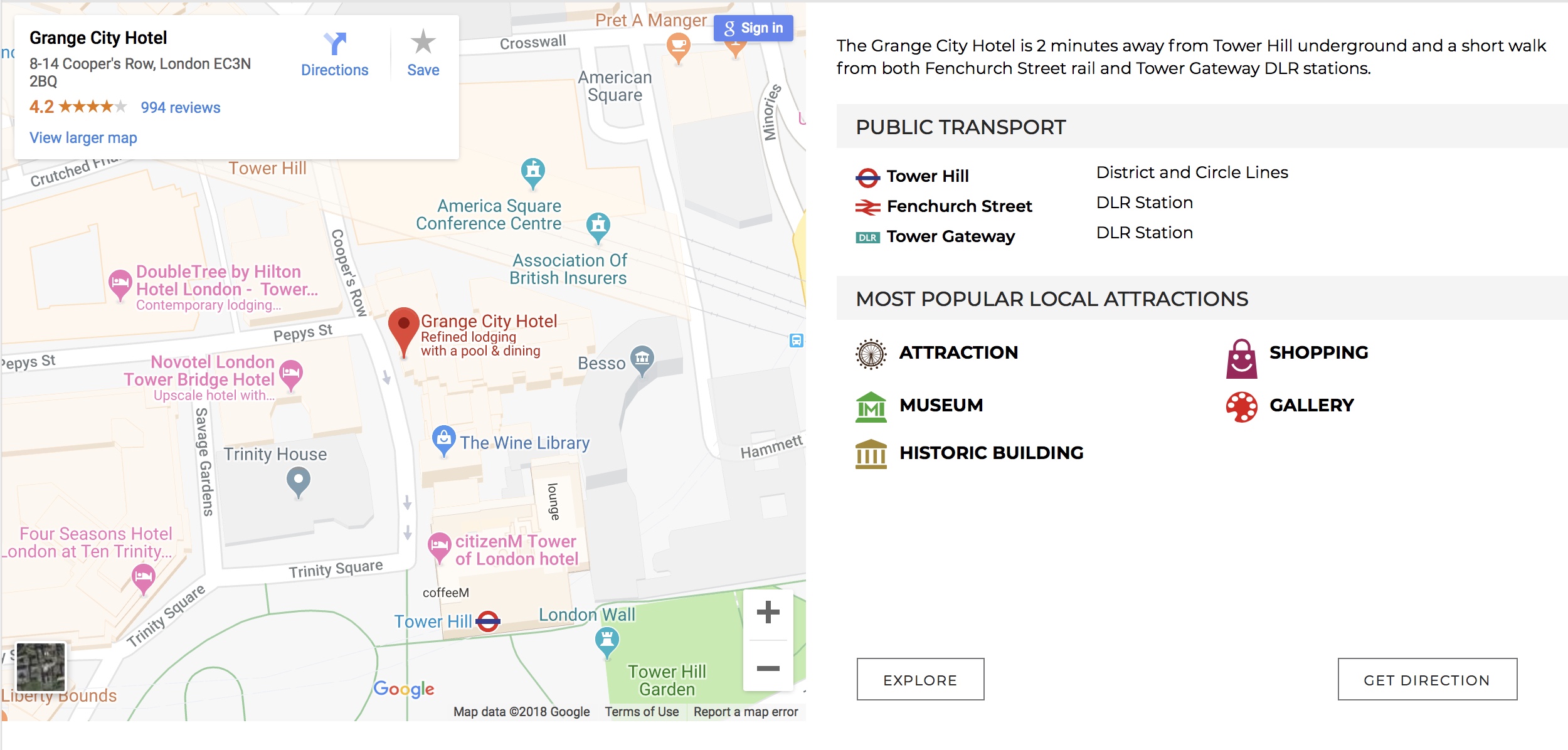
We are delighted to announce details of the 4th BUS Birdshot Uveitis Day on Saturday 17th November 2018. It will be held at the Grange City Hotel, 8-14 Coopers Row, London EC3N 2BQ, close to Tower Hill Underground station and Fenchurch Street mainline rail station. This educational day is intended for people with birdshot uveitis, their family members, health professionals who treat people with birdshot, those who research birdshot, or for anybody who wants to learn more about the condition.
This year we have a really exciting programme planned, and as well as our fabulous UK team of birdshot uveitis expert speakers we are also honoured to welcome Professor Jennifer Thorne, Cross Family Professor of Ophthalmology at the Wilmer Eye Institute, Johns Hopkins Baltimore, where she is also chief of the Division of Ocular Immunology, and Dr Marina Mesquida who is an ophthalmologist clinician scientist, now working for Roche Pharma research and early development as Translational Medicine Leader in Ophthalmology. We are also extremely fortunate to have Professor Russell Foster, who is a professor of circadian neuroscience, the Director of the Nuffield Laboratory of Ophthalmology and the Head of the Sleep and Circadian Neuroscience Institute, Oxford University, for our keynote talk about sleep and how problems with sleeping (or rather lack of it) affect our health.
A two-course buffet lunch, tea and coffee will be provided. The day will close at 5.00pm but we are also planning to organise an informal social get-together afterwards in a nearby pub or bar, to allow even more time for chatting. Details will be announced nearer the day.
Below is the outline programme for the day:
BIRDSHOT DAY NO 4 PROGRAMME
Saturday 17th November 2018 from 10.00am – 5.00pm with registration and coffee from 9.15am.
SESSION 1 Chaired by Professor Miles Stanford
Birdshot ABC: to include information about birdshot uveitis, the immune system and getting the most out of your eye appointment. Speakers to include: Mr Richard Lee (Bristol and Moorfields), Miss Laura Steeples (Manchester) and Mr Greg Heath (York).
SESSION 2 Chaired by Professor Alastair Denniston
Overview on the world of birdshot research, with Professor Alastair Denniston and Professor Andrew Dick interviewing Professor Jennifer Thorne and Dr Marina Mesquida.
SESSION 3 Chaired by Professor Andrew Dick
Sleep and how it affects your health and immune system: Professor Russell Foster, Professor of Circadian Neuroscience, Oxford University.
SESSION 4 Introduced by Annie Folkard
Living with sight loss: practical tips and apps that may help increase independence if you have started to lose vision. Speakers: Julian Jackson, Chen Yogev from Orcam and Preeti Singla, an expert low vision optometrist.
SESSION 5 Chaired by Professor Alastair Denniston
BUS/Fight for Sight funded research: short update on what we have discovered so far. Speakers include: Dr Graham Wallace, Dr Omar Mahroo, Mr Mark Westcott, Dr Colin Chu and Professor Philip Murray.
SESSION 6 Chaired by Professor Philip Murray
Birdshot – treatment and trials update. Have your say with a professionals and patients panel. Speakers to include: Professor Andrew Dick, Professor Jennifer Thorne and Dr Marina Mesquida, Professor Miles Stanford.
QUESTION TIME Chaired by Professor Andrew Dick. The birdshot panel answers your questions.
AFTER-EVENT SOCIAL We are going to have a social after the main event in a local bar or pub. Please let us know if you think you might like to attend this and we will send you more information about it later. We are just trying to judge numbers at the moment.
As well as the talks, on the day you will be able to network and socialise with our ‘Birdshot Community’ made up of professionals, people with birdshot and family members. You will be able to:
- Learn more about birdshot and the immune system
- Learn how to get the most from your eye clinic appointment
- Learn more about the impact of sleep on your immune system and health
- Meet experts in the field of birdshot and vision impairment
- Meet other patients with a birdshot diagnosis
- Ask questions about birdshot
- Find out about new treatments and research
As before, we will have a range of exhibitors attending. There will also be interactive sessions in the breaks where you can learn more about the immune system and also talk to people involved in birdshot research.
Please register on line to reserve your place, or print off the Birdshot Day Registration Form 2018 and send it to BUS, PO Box 64996, London SW20 2BL, or return it by email to info @ birdshot.org.uk.
This event is being organised by BUS and members of the National Birdshot Research Network. We are particularly grateful to Professor Andrew Dick, Professor Alastair Denniston and Karen Bonstein for their help with developing the programme. We are extremely fortunate to have the continued support of a dedicated group of clinicians and researchers who form the heart of the National Birdshot Research Network.
BUS very much looks forwards to meeting you all on Saturday 17th November 2018.
Annie
for Team Birdshot
Email: info @ birdshot. org.uk
Book your places now!
As before, the conference, including lunch, is free, but we do require a £20 refundable registration deposit (plus £1 non-refundable administration fee to pay for postage and Paypal fees). Your registration fee can be returned when you attend the Day, but if you choose to donate your registration fee to help BUS develop the next Birdshot Day, we very warmly welcome this. You can pay your registration fee by using the button below (debit and credit card & PayPal), or by sending a cheque by post to BUS, PO Box 64996, London SW20 2BL.
If you are claiming benefits or on a pension, we will waive the deposit as we do not want to prevent people attending due to financial constraints. Please select this option on the dropdown PayPal button.
Accommodation
If you want overnight accommodation, the Grange City Hotel has offered us a concessionary rate. Please note that to obtain the special rate, your hotel booking must be made at least one month in advance of the event, as nearer to the date prices will unfortunately go up. We have been offered a special rate including English breakfast and complimentary upgrade to executive room where available for:
- Friday 16th November – £119 + vat
- Saturday 17th November – £139 + vat
The reference people should quote when booking via phone (020 7863 3700) or email city.reservations@grangehotels.com is CCT1711090.



{kind=link}
{kind=link}